

Mycoplasma Genitalium: Symptoms, Transmission, Diagnosis & Treatment
Mycoplasma Genitalium: Symptoms, Testing, Treatment
Mycoplasma genitalium (Mgen) is one of the most underdiagnosed sexually transmitted infections. It’s sneaky many people have it without symptoms but when it causes problems, it can mimic BV, cause persistent urethritis, or lead to serious complications like pelvic inflammatory disease (PID).
If you’ve had recurrent vaginal symptoms that don’t fully respond to BV or yeast treatment, Mgen might be worth asking your clinician about. This guide covers what Mgen is, how it shows up in women, how it overlaps with BV, testing options, and current treatment guidelines (updated for 2026). It’s not personal medical advice, but it can help you advocate for comprehensive testing.
What is Mycoplasma genitalium?
Mycoplasma genitalium is a tiny bacterium that infects the genital and urinary tracts. Unlike most bacteria, it:
Lacks a cell wall (makes it resistant to some antibiotics).
Lives inside cells (harder to detect).
Spreads primarily through sexual contact (vaginal, anal, possibly oral). brightonsexualhealth
Key facts:
Affects 1–3% of sexually active adults (higher in some groups).
Often asymptomatic (up to 50–80% of cases).
Causes treatment‑resistant urethritis and cervicitis.
Increasing antibiotic resistance worldwide. cleavlandclinic
Mgen is not the same as BV (microbiome imbalance), but they co‑occur frequently and share symptoms.
Mgen symptoms in women
When symptomatic, Mgen often causes nonspecific vaginal or urinary symptoms:
Common symptoms
Increased vaginal discharge (yellowish, sometimes odorless).
Burning with urination (urethritis).
Pain during sex (cervicitis).
Bleeding between periods or after sex.
Lower abdominal/pelvic pain.
Itching or irritation (vulva/urethra). evvy
Silent infections
Most women with Mgen have no symptoms, making routine screening challenging.
How Mgen overlaps with BV and other conditions
Mgen symptoms mimic common vaginal issues:
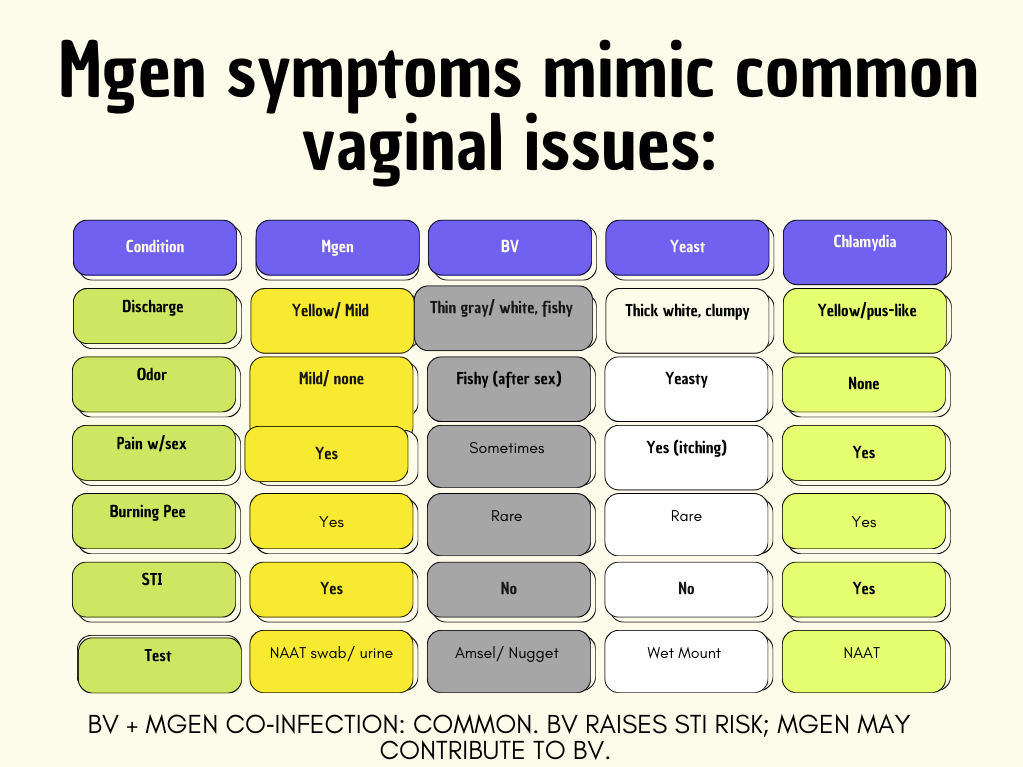
Recurrent cervicitis: Mgen is a leading cause in women who keep returning with “BV” that doesn’t fully resolve. [cd
Why Mgen is hard to diagnose
No routine screening
Not in standard STI panels (unlike chlamydia/gonorrhea).
Expensive/specialized NAAT tests.
No FDA‑approved urine test for women (swabs preferred). testing
When to test
CDC recommends Mgen testing for: cdc
Persistent/recurrent urethritis/cervicitis after chlamydia treatment.
PID (pelvic inflammatory disease).
Recurrent BV/yeast not responding to treatment.
Clinician should consider if:
Sexually active with new/multiple partners.
Persistent symptoms despite negative chlamydia/gonorrhea. cdc
How Mgen is tested
Vaginal/cervical swab (women)
NAAT (nucleic acid amplification test) detects Mgen DNA.
High sensitivity/specificity (>95%).
Self‑collect possible in some clinics. evvy
Urine (first‑catch)
Less sensitive for women than swabs.
Acceptable if pelvic exam not feasible.
Resistance testing
Macrolide resistance (azithromycin) now common (>40%).
Moxifloxacin resistance emerging.
Guides treatment when available.
Test of cure: 3–4 weeks post‑treatment for persistent symptoms.
Mgen treatment (2026 guidelines) onlinelibrary.wiley
Mgen is tricky due to rising resistance. CDC/European guidelines emphasize resistance‑guided therapy.
Preferred: Resistance testing available
Doxycycline 100 mg twice daily x 7 days (reduces bacterial load).
Test for macrolide resistance.
Azithromycin (if sensitive): High‑dose extended course.
Moxifloxacin 400 mg daily x 7 days (if resistant).
No resistance testing
CDC 2021–2026 recommendation:
Doxycycline 100 mg BID x 7 days + Moxifloxacin 400 mg daily x 7 days.
Cure rates: >90% with proper resistance‑guided therapy.
Partner treatment
Yes treat all recent sexual partners to prevent ping‑pong reinfection.
Same regimen (doxycycline + moxi if needed).
Abstain or condoms until both complete treatment + test of cure.
Complications if untreated
Short‑term
PID (10–20% risk).
Cervicitis/urethritis.
Infertility risk from tubal scarring.
Long‑term
Chronic pelvic pain.
Ectopic pregnancy risk.
Preterm birth (if pregnant).
Prevention
Condoms (imperfect reduces but doesn’t eliminate risk).
Partner testing/treatment.
Fewer partners reduces exposure.
Routine STI screening if high‑risk.
Frequently asked questions
Q: Is Mgen the same as BV?
No. BV = microbiome imbalance. Mgen = STI. They co‑occur and share symptoms (discharge, odor). Test both if recurrent.
Q: Why isn’t Mgen routinely tested?
Costly, specialized NAAT. Not FDA urine test for women. Reserve for persistent symptoms post‑chlamydia treatment or PID.
Q: Can Mgen cause recurrent BV?
Yes Mgen disrupts microbiome, raises STI susceptibility. Treat both for clearance.
Q: What if azithromycin fails?
Resistance common (>40%). Test partners, retreat with moxifloxacin. Test of cure mandatory.
Q: Asymptomatic partners need treatment?
Yes reinfection common without partner treatment.
Q: Pregnancy risks?
High miscarriage, preterm birth. Test/treat promptly.
Key takeaways
Mgen = emerging STI mimicking BV, urethritis, PID.
Test if recurrent symptoms post‑standard treatment.
Doxycycline + moxifloxacin for resistance. Partner treatment essential.
BV/Mgen co‑occur test comprehensively.
Advocate: “I’ve had recurrent BV/yeast. Can we test for Mycoplasma genitalium?” Print this guide.
Resources and Sources:
https://my.clevelandclinic.org/health/diseases/mycoplasma-genitalium
https://www.evvy.com/blog/mycoplasma-genitalium
https://www.testing.com/tests/mycoplasma/
https://www.cdc.gov/std/treatment-guidelines/mycoplasmagenitalium.htm
About the Author
Becky Freeman is the founder of BVTalks® and Bee Vee Clean. She focuses on women’s intimate health, vaginal microbiome education, and creating practical, easy-to-understand content for everyday care.
Medical Disclaimer
This content is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any condition. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider if you have questions about your health or symptoms.