

Aerobic Vaginitis (AV) vs. Bacterial Vaginosis (BV): They Are Not the Same Thing
If you've been living with recurring vaginal symptoms discharge, odor, burning, irritation and antibiotics keep failing you, there is a possibility that has likely never been raised in your doctor's office: you might not have BV at all.
Aerobic Vaginitis, or AV, is a vaginal condition that is frequently mistaken for bacterial vaginosis. It causes many of the same symptoms, it is diagnosed in the same exam room, and yet it is a completely different disease caused by completely different bacteria which means it requires completely different treatment. Giving someone with AV a metronidazole prescription is like giving someone with a broken arm a cast for the wrong leg. It will not help, and the underlying problem gets worse.
This post breaks down exactly what makes AV and BV different, why they get confused, and what it means for your treatment.
What Is Bacterial Vaginosis (BV)?
BV is the most common vaginal condition in women ages 15–44. It is caused by an overgrowth of anaerobic bacteria organisms that thrive without oxygen following a decline in the protective Lactobacillus bacteria that normally dominate the healthy vagina.
The key bacteria associated with BV include:
Gardnerella vaginalis the primary architect of vaginal biofilm in BV
Atopobium vaginae (Fannyhessea vaginae)
Prevotella species
Mobiluncus species
Mycoplasma hominis
BV raises vaginal pH above 4.5 and produces the characteristic thin, grayish-white discharge with a fishy odor that intensifies after sex. It is diagnosed using the Amsel criteria or Nugent scoring, and treated primarily with metronidazole or clindamycin.
What Is Aerobic Vaginitis (AV)?
Aerobic Vaginitis was formally described as a distinct condition by Professor Gilbert Donders in 2002, though it had been causing misdiagnosed suffering in women long before that. Unlike BV which is caused by anaerobic (oxygen-avoiding) bacteria AV is caused by an overgrowth of aerobic bacteria, meaning organisms that thrive with oxygen.
The bacteria most commonly responsible for AV include:
Escherichia coli (E. coli) the most common AV pathogen, normally found in the gut
Group B Streptococcus (GBS / Streptococcus agalactiae) also significant in pregnancy complications
Staphylococcus aureus* including MRSA strains in severe cases
Enterococcus faecalis* another gut-origin bacteria
Klebsiella pneumoniae*
These are not the quiet, low-grade anaerobes of BV. These are robust, often aggressive bacteria that trigger real immune responses meaning AV comes with inflammation in a way that BV typically does not.
How Are BV and AV Similar?
This is exactly why they get confused so often:
Both cause abnormal vaginal discharge
Both cause vaginal odor
Both raise vaginal pH above 4.5
Both represent a disruption of normal Lactobacillus dominance
Both are more common in sexually active women
Neither is classified as a sexually transmitted infection (though sexual activity influences both)
Both can be asymptomatic in some women
When a patient walks into an office with discharge and odor, the reflex is often to diagnose BV. But if AV is present instead or alongside BV in a mixed infection the standard BV treatment will fail entirely.
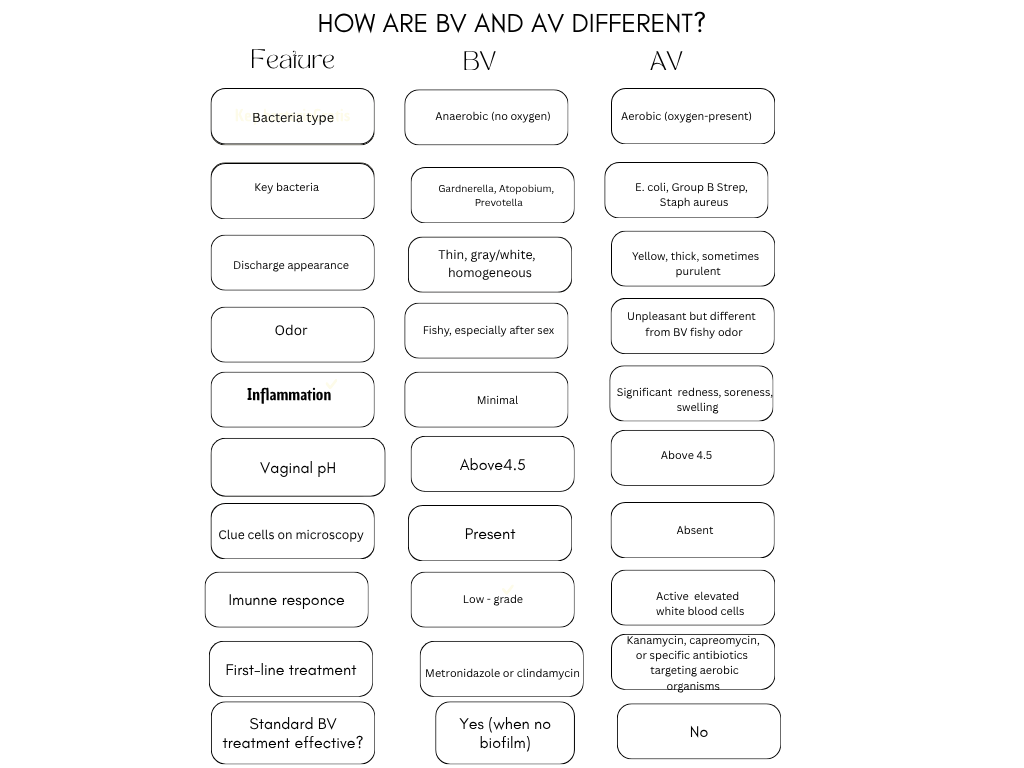
The inflammation piece is crucial. AV triggers a significant immune response the vaginal walls become red, irritated, and swollen. Women with AV often describe burning and soreness more prominently than women with BV, and the discharge tends to be yellower and thicker rather than the thin grayish discharge of BV.
What Are AV Strains and Why Do They Matter?
The aerobic bacteria behind AV are not random they are organisms that typically originate from the gastrointestinal tract and make their way into the vaginal environment through proximity (the anus and vagina are anatomically close), poor wiping technique, contaminated water, or sexual activity.
E. coli is the most studied AV pathogen. It produces toxins that directly damage vaginal epithelial cells, triggers intense inflammation, and can ascend to cause UTIs, kidney infections, and in pregnant women, very serious pregnancy complications.
Group B Streptococcus (GBS) is particularly significant because it is routinely screened for during pregnancy GBS colonization can be passed to the newborn during delivery and cause life-threatening neonatal sepsis. What many women don't realize is that GBS as part of AV can cause ongoing vaginal symptoms outside of pregnancy too.
Staphylococcus aureus in the vagina is less common but more serious especially antibiotic-resistant strains. It produces toxins and enzymes that break down tissue and can cause severe inflammation.
Mixed Infections: When BV and AV Occur Together
Research by Professor Donders and colleagues has shown that BV and AV can coexist simultaneously in the same woman a condition sometimes called desquamative inflammatory vaginitis in its most severe form, or simply documented as a mixed BV/AV infection.
This is particularly relevant for women with treatment-resistant symptoms. If you have both BV-associated anaerobes AND aerobic AV bacteria present at the same time, treating only one population will leave the other behind. A full picture of your vaginal bacterial community ideally through PCR molecular testing is the only way to know what you're actually dealing with.
How Is AV Diagnosed?
Standard BV testing (Amsel criteria, Nugent score, pH testing) does not adequately capture AV. Proper AV diagnosis requires:
Microscopy with specific attention to white blood cells (lactobacillary grade, parabasal cells, and leukocyte count)
Vaginal culture to identify the specific aerobic organism present
PCR-based molecular testing for comprehensive bacterial identification services like Evvy or Juno Diagnostics can detect AV-associated bacteria specifically
If your provider only tests for BV and gives you metronidazole without improvement, it is worth asking specifically about AV testing.
How Is AV Treated?
Because AV is caused by aerobic bacteria, it requires antibiotics that target aerobic organisms which are very different from BV antibiotics:
Kanamycin vaginal creamconsidered one of the most effective AV treatments in European research
Clindamycin has some activity against certain AV bacteria but is more of a BV drug
Topical steroids (like hydrocortisone) may be used alongside antibiotics in severe cases to reduce inflammation
Estrogen cream particularly in perimenopausal or postmenopausal women, since declining estrogen contributes to AV susceptibility
Treating the specific organism E. coli, GBS, and Staph aureus each have different antibiotic sensitivities, which is why culture-based testing matters
Metronidazole the standard BV drug has no meaningful activity against aerobic bacteria and will not treat AV.
AV and Pregnancy: A Serious Concern
AV during pregnancy carries significant risks that deserve their own emphasis:
Preterm birth and premature rupture of membranes
Neonatal GBS infection potentially life-threatening for newborns
Chorioamnionitis (infection of amniotic membranes)
Postpartum endometritis
Pregnant women with symptoms of vaginal infection who are not responding to standard BV treatment should specifically request AV screening. The stakes are high enough that a comprehensive vaginal evaluation is worth pushing for.
Lifestyle Support for Both BV and AV
Whether you are dealing with BV, AV, or both, these foundational steps support vaginal health across the board:
Wipe front to back, always this is especially important for AV since gut bacteria like E. coli are a primary source
Wear 100% cotton underwear to reduce moisture and heat that encourage bacterial overgrowth
Shower after swimming pool water and its bacteria can disrupt both vaginal pH and bacterial balance
Use pH-balanced, fragrance-free cleansers on the external vulva only never inside the vagina
Stay well-hydrated to support urinary tract flushing and overall immune function
Follow up with probiotics after any antibiotic course to help restore Lactobacillus dominance
Frequently Asked Questions
Can I have AV without any symptoms?
Yes. Like BV, AV can be asymptomatic in some women, particularly in the early or low-grade stages.
Is AV more serious than BV?
In some ways, yes AV triggers more active inflammation and is associated with significant pregnancy complications. However, both conditions deserve proper diagnosis and treatment.
Can AV go away on its own?
Unlike mild BV, AV is less likely to resolve without treatment due to the inflammatory nature of the aerobic bacteria involved. Always seek medical care for suspected AV.
Does my sexual partner need treatment for AV?
Current guidelines do not routinely recommend partner treatment for AV, but because aerobic bacteria can be exchanged through sexual activity, barrier protection during active treatment is generally advisable.
“This article is based on current medical guidance and research from the following trusted sources:”
Resources & Sources
Donders, G.G.G., et al. (2002).- Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis. BJOG: An International Journal of Obstetrics and Gynaecology.
Centers for Disease Control and Prevention (CDC)- Vaginal Health: cdc.gov
National Institutes of Health (NIH) PubMed: pubmed.ncbi.nlm.nih.gov
American College of Obstetricians and Gynecologists (ACOG): acog.org
Donders, G., et al. (2011).- Aerobic vaginitis in pregnancy. BJOG.
Have you ever been treated for BV repeatedly without success? It might be time to ask your doctor about AV. Share your story in the comments or email this is a safe space for every question.
Author
Becky Freeman is the founder of BVTalks®. She focuses on women’s intimate health, vaginal microbiome education, and creating practical, easy-to-understand content for everyday care.
Disclaimer: This post is for educational purposes only and is not a substitute for professional medical advice. Always consult your healthcare provider for diagnosis and treatment.